
Medical finger probes
Best for clinical decisions when they are FDA-cleared or otherwise regulated, paired with the right sensor, and used on a warm, well-perfused site.
Not always “best.” Often “best understood.”
A plain-English guide to SpO2, why some monitors perform better than others, when the number misleads, and why oxygen care in babies is a different universe.
The quick read
For many healthy adults at sea level, a finger pulse oximeter often reads around 95-100%. Lower values can be normal for some people with known lung or heart disease, at altitude, or during monitored newborn transition. But a reassuring number can still be wrong in carbon monoxide poisoning, poor circulation, abnormal hemoglobin, motion, cold fingers, nail polish, and some skin tones.
Trust the trend, the person, and the context. If symptoms and the number disagree, believe the person and seek clinical help.
Accuracy
Hospital-grade devices are not all equal, and consumer wellness devices are a separate category. The biggest practical challenges are low perfusion, movement, darker skin pigmentation, abnormal hemoglobin, and signal noise.
Best for clinical decisions when they are FDA-cleared or otherwise regulated, paired with the right sensor, and used on a warm, well-perfused site.
Masimo deserves special attention because its signal extraction technology has a long clinical evidence base in motion and low-perfusion settings. It is reasonable to present Masimo as a leading benchmark, while avoiding magical claims.
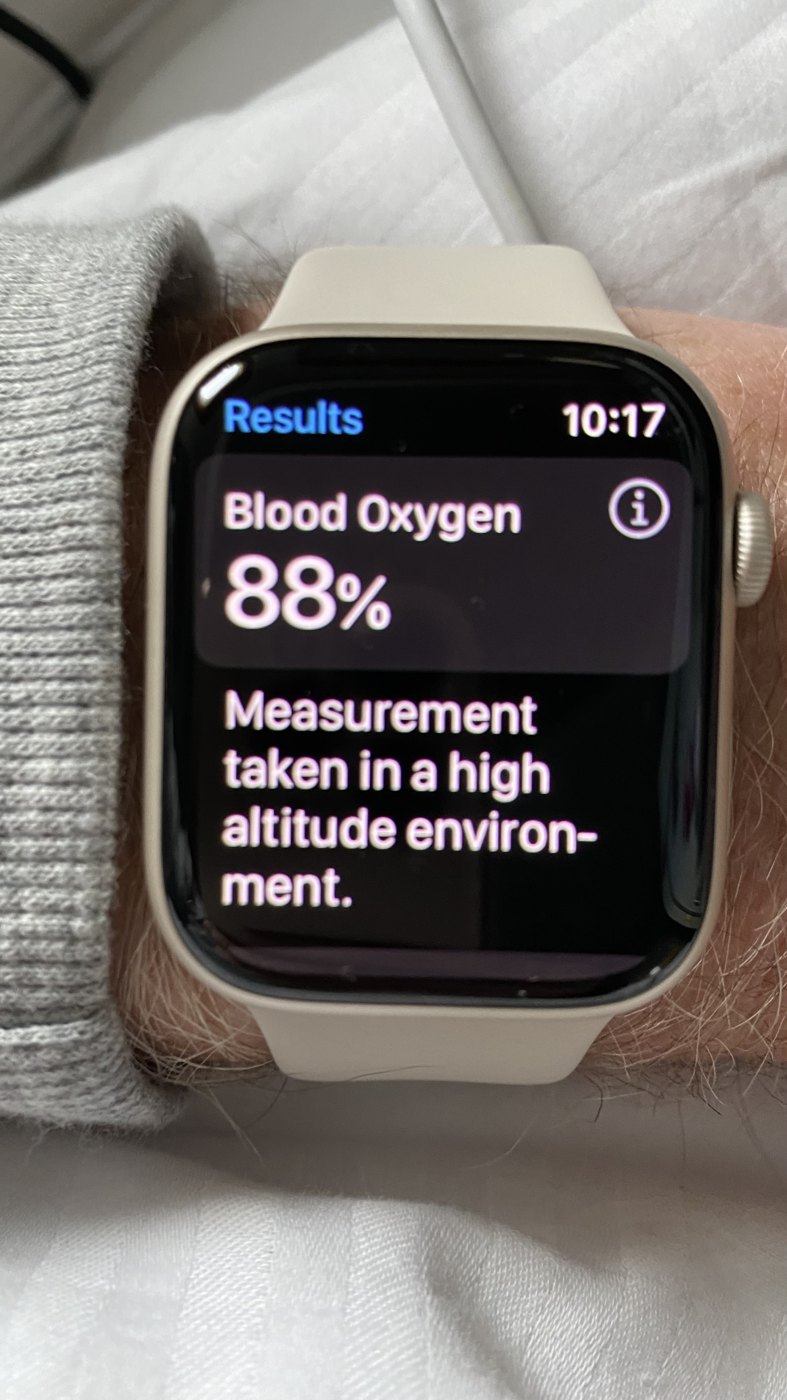
Useful for trends, sleep, altitude, and wellness. Less ideal for urgent clinical decisions because wrist and ring signals face movement, fit, temperature, and algorithm limits.
The FDA says current evidence shows performance differences between lighter and darker skin pigmentation, and it proposed updated recommendations in January 2025 to improve performance across skin tones. Darker skin can increase the risk of “occult hypoxemia,” where SpO2 looks acceptable while arterial oxygen saturation is lower.
Masimo accused Apple of using its blood-oxygen technology and trade secrets. The dispute led Apple to disable or redesign blood-oxygen features on some U.S. Apple Watch models. By April 2026, reporting indicated the ITC would not continue reviewing Masimo petitions over Apple’s redesigned workaround, though related appeals and commercial disputes may continue.
Our bias, stated plainly
Masimo earned that position by obsessing over the hard cases: motion, low perfusion, weak signals, neonatal monitoring, remote continuous monitoring, and the messy real-world situations where a cheap clip can look confident while being wrong. No device is perfect, and clinical judgment still wins, but Masimo has a serious evidence base and a long record of pushing pulse oximetry forward.
How it works
A standard pulse oximeter shines red and infrared light through tissue. Oxygen-rich and oxygen-poor hemoglobin absorb those wavelengths differently. The device focuses on the pulsing part of the signal, because arterial blood pulses and most other tissue does not.
The displayed SpO2 is not directly measured oxygen gas. It is an algorithmic estimate of hemoglobin saturation.
Anesthesia and ICU
Pulse oximetry became one of anesthesia’s great safety advances because it gave clinicians a continuous, audible warning that oxygenation was drifting before the patient looked blue. In the 1980s and 1990s, it joined capnography, blood pressure, ECG, temperature, and direct clinical vigilance as part of modern basic monitoring.
Takuo Aoyagi’s 1970s invention made pulse oximetry possible. William New, an anesthesiologist with engineering training at Stanford in Palo Alto, helped bring the technology into routine anesthesia by co-founding Nellcor in 1981. Nellcor’s early N-100 bedside oximeter appeared in 1983 and quickly became a favored operating-room monitor.
Pulse oximetry tells you oxygenation is falling. Continuous end-tidal carbon dioxide monitoring tells you whether breaths are reaching the lungs. That is why capnography is so important for detecting a misplaced endotracheal tube, disconnection, apnea, or severe hypoventilation, often before the oxygen saturation has had time to fall.
Modern anesthesia mortality fell by roughly an order of magnitude over the broader safety era. It was not pulse oximetry alone: training, standards, safer drugs, checklists, capnography, better machines, and recovery-room care all mattered. But pulse oximetry plus continuous CO2 monitoring is one of the clearest examples of technology turning silent deterioration into an early alarm.
The oxygen curve
The oxygen-hemoglobin dissociation curve is the relationship between oxygen pressure in the blood and how full hemoglobin is. The top is flat: big PaO2 changes may barely move SpO2. The middle is steep: small oxygen drops can cause large saturation drops.
Fever, exercise, higher CO2, acidosis, and higher 2,3-BPG help hemoglobin unload oxygen to tissues.
Cold, low CO2, alkalosis, fetal hemoglobin, carbon monoxide, and some hemoglobin variants make hemoglobin cling to oxygen.
CaO2 is roughly: hemoglobin x 1.34 x saturation + dissolved oxygen. Severe anemia can leave SpO2 normal while total oxygen carried is dangerously low.
What changes oxygen
Device types
Worth knowing
Masimo W1 Medical received FDA 510(k) clearance for adult over-the-counter and prescription use as a medical watch providing continuous real-time SpO2 and pulse rate. In 2024, Masimo also announced FDA clearance for connectivity with Masimo SafetyNet, positioning it more as a clinical telemonitoring wearable than a fitness-watch oxygen feature.
Beyond ordinary SpO2
Masimo’s rainbow platform uses multi-wavelength sensors to estimate additional blood constituents and physiologic parameters, including noninvasive total hemoglobin trend monitoring (SpHb), carboxyhemoglobin (SpCO), methemoglobin (SpMet), oxygen content (SpOC), oxygen reserve index (ORi), perfusion index, and pleth variability. This is especially interesting in anesthesia, emergency medicine, critical care, transfusion decisions, carbon monoxide exposure, and methemoglobinemia risk.
Important caveat: these measurements can add trend visibility, but Masimo itself notes that SpHb and SpMet are not intended to replace laboratory blood testing, and SpCO is not the sole basis for carbon monoxide diagnosis or treatment.
Buying links
BestOximeters.com may later use affiliate links to retailers or manufacturers, including Amazon or Masimo if a suitable program is agreed. The editorial position stays separate: medical usefulness, validation, and limitations matter more than commission.
Real-world examples
Oximetry is not one device or one setting. The same number may appear on a bedside monitor, a transport monitor, a finger clip, or a watch, but each reading sits inside a different clinical situation, signal quality, and decision pathway.



Oxygen concentrators
An oxygen concentrator does not store oxygen like a cylinder. It pulls room air through filters and molecular sieves, removes much of the nitrogen, and delivers oxygen-enriched gas through tubing, usually by nasal cannula. The prescription matters: flow rate, hours of use, target saturation, sleep/exertion needs, and backup plans should be individualized.
Runs from mains power, usually provides continuous flow, and is common for overnight or long-duration home oxygen. It is heavier and less portable, but often more reliable for higher flow needs.
Battery-powered for movement and travel. Many deliver pulse-dose oxygen triggered by inhalation; some offer limited continuous flow. Fit matters because pulse-dose may not suit every patient, especially during sleep or rapid shallow breathing.
Cylinders store compressed oxygen and are useful as backup or for outings. Liquid oxygen can support higher portable oxygen needs where available, but supply systems vary by country and provider.
Ask whether the prescription requires continuous flow or pulse-dose, whether oxygen is needed during sleep, exercise, altitude, or illness, what alarms mean, and what to do during power cuts.
Too much oxygen
Oxygen is a drug. The goal is usually enough oxygen to prevent tissue hypoxia, not the highest number possible. Over-oxygenation can matter in newborns, adults in intensive care, people with COPD or CO2 retention risk, divers, and patients receiving hyperbaric oxygen.
Prolonged high oxygen exposure can irritate and injure the lungs, causing cough, chest discomfort, absorption atelectasis, inflammation, pulmonary edema, and ARDS-like injury in severe cases.
At high oxygen partial pressures, especially in hyperbaric settings or diving, oxygen toxicity can cause visual changes, tinnitus, nausea, twitching, anxiety, dizziness, and generalized seizures.
Some patients with COPD, obesity hypoventilation, neuromuscular weakness, or sedative/opioid exposure can retain carbon dioxide. Oxygen may improve SpO2 while ventilation remains inadequate.
Premature infants are uniquely vulnerable to oxygen-related eye and lung injury, including retinopathy of prematurity and bronchopulmonary dysplasia. This is why neonatal oxygen is carefully targeted.
Hyperbaric oxygen is useful for selected conditions such as decompression sickness, carbon monoxide poisoning, gas embolism, and some wound/radiation injuries. It should be delivered by trained teams because pressure increases both benefit and toxicity risk.
Oxygen itself is not flammable, but it makes other materials ignite more easily and burn faster. Keep oxygen away from smoking, open flames, gas stoves, oils, petroleum jelly, aerosols, hair dryers, heaters, and sparking equipment.
Newborn oxygen
Before birth, fetal oxygen saturation is much lower than adult oxygen saturation. After birth, oxygen levels normally rise over several minutes as the lungs open and placental circulation closes. Too little oxygen is dangerous, but too much oxygen can also injure premature eyes and lungs.
Before birth, the placenta does the gas exchange, the lungs are high-resistance, and blood can bypass them through the foramen ovale and ductus arteriosus. After the first effective breaths, lung blood flow rises, oxygen levels climb, and those fetal shortcuts begin to close.
Concerning oxygen deprivation may first show as fetal bradycardia: a slow fetal heart rate on monitoring. Clinicians watch the heart rate because a stressed baby often shows it there first.
Premature lungs may lack surfactant, the substance that keeps air sacs open. Antenatal steroids can speed lung maturity; after birth, support may include CPAP, ventilation, caffeine, oxygen, and surfactant.
Bronchopulmonary dysplasia is chronic lung disease of prematurity, linked to immature lungs plus prolonged oxygen and respiratory support. Modern care tries to use enough oxygen, pressure, and volume, but no more than needed.
NEHI kids
NEHI stands for neuroendocrine cell hyperplasia of infancy. It is part of childhood interstitial lung disease, or chILD, and usually appears in the first months to two years of life. It can seem “commoner” now because clinicians, CT imaging, and specialist chILD services are uncovering cases that previously may have been labelled as asthma, recurrent infections, unexplained tachypnea, or just “slow to grow.” Families often meet it through a confusing pattern: a baby who breathes fast, works hard, has low oxygen saturations, and does not behave like ordinary asthma.
Common features include persistent fast breathing, chest retractions, crackles heard with a stethoscope, lower oxygen levels, poor weight gain, and worse dips during sleep or viral infections. Some children are first treated for asthma or repeated chest infections, but NEHI often does not respond much to bronchodilators or steroids.
The oxygen story matters because breathing itself burns calories. Supplemental oxygen can reduce strain and help growth, even when it is used mainly at night, during illness, or with activity.
Doctors usually rule out infection, heart disease, cystic fibrosis, immune problems, aspiration, and other causes. High-resolution CT often shows a typical pattern of ground-glass change and air trapping, sometimes enough for a clinical diagnosis. Infant lung-function testing or lung biopsy may be needed when the picture is not classic.
Care is mainly supportive: oxygen, nutrition, infection prevention, vaccines, and pediatric respiratory follow-up. There is no simple “NEHI medicine,” and oral steroids have not shown consistent benefit for most children.
Most children improve as they grow. Many gradually reduce or stop oxygen, though the timeline varies and some older children still need oxygen for sleep, illness, altitude, or exertion.
Causes of low oxygen
Asthma, COPD, emphysema, bronchiectasis, cystic fibrosis, mucus plugging, bulbar palsy, aspiration, frailty, cachexia, motor neuron disease.
Pneumonia, viral illness, atypical infection, mycoplasma, chemical pneumonitis, interstitial lung disease, NEHI and other chILD conditions, silicosis, asbestosis, TB, cancer, mesothelioma.
Total lung collapse, major atelectasis, severe pneumonia, pulmonary edema, congenital or acquired shunts. Shunt physiology can be stubborn: oxygen may help less than expected.
Pneumothorax, pleural effusion, chest wall problems, neuromuscular weakness, severe obesity hypoventilation, postoperative splinting.
Anemia, sickle cell disease, thalassemias, carbon monoxide poisoning, methemoglobinemia, sulfhemoglobinemia, and rare hemoglobin variants.
Altitude, smoke inhalation, low-oxygen confined spaces, carbon monoxide, cyanide in fires, and industrial or chemical exposures.
Sources
This site is educational and cannot diagnose or treat illness. Urgent breathlessness, blue/gray lips, confusion, chest pain, severe drowsiness, carbon monoxide concern, or a child/newborn who looks unwell should be treated as urgent.
{kind=link}